Access economics arrive: Lilly walks away from a PBS deal for Mounjaro, Wegovy stays in the queue, and the private-pay market holds the GLP-1 line
This period marks the shift from "shortage and launch excitement" into access economics and channel discipline. The defining Australian event is the Mounjaro stand-off: the PBAC recommended tirzepatide for adults with inadequately controlled type 2 diabetes, but Eli Lilly declined to proceed with PBS listing under the proposed reimbursement conditions — a decision the manufacturer and Medicines Australia framed as evidence of a "broken" reimbursement system. The practical effect is that private-pay tirzepatide remains dominant, Ozempic and Trulicity stay as the PBS GLP-1 options for diabetes, and PBS access for obesity medicines looks set to move through narrow, priority-group pathways rather than a broad mass-market subsidy. Around this, Wegovy remains recommended (for established cardiovascular disease with obesity) but not yet listed; the Ozempic shortage has resolved while the 1.5 mL starter pen runs out its PBS Supply Only transition to 1 June 2026; the Trulicity shortage continues to 30 June 2026; Lilly's Q1 2026 results confirm Mounjaro and Zepbound are still driving global incretin growth; and the consumer GLP-1 "support supplement" adjacency is going mainstream.
The PBS line in the sand
PBAC recommended tirzepatide; Lilly declined to list under the proposed terms. Obesity-medicine subsidy is being steered toward narrow priority groups, not broad consumer access.
From scarcity to discipline
Ozempic supply has resolved, but a 1.5 mL→3 mL pen transition runs to 1 June and Trulicity stays short to 30 June. Counselling accuracy, not scarcity, is now the pharmacy task.
The support stack goes mainstream
Protein, fibre, probiotics and micronutrient "GLP-1 support" content is now mainstream. Pharmacy holds the strongest permission space for compliant, pharmacist-guided bundles.
Three near-term signals: (1) whether Lilly re-engages on Mounjaro PBS terms or holds the private-pay line; (2) movement on the Wegovy eCVD-with-obesity listing arrangements after its PBAC recommendation; (3) the 1 June Ozempic pen transition and the 30 June Trulicity shortage end-date — recheck both TGA pages before acting.
| Domain | Activity Level | Top Signal | Australian Impact |
|---|---|---|---|
| Regulatory & Access | ● High | Mounjaro PBS stand-off; Wegovy recommended, not listed | Direct — defines access economics |
| Supply & Integrity | ● High | Ozempic resolved; pen transition to 1 Jun; Trulicity short to 30 Jun | Direct — dispensing transitions live |
| Generic & Patent | ● Low | No new Australian generic entry; global backdrop only | Global-pathway — AU secondary patents to 2030s |
| Clinical Pipeline | ● Medium | Lilly Q1 2026 incretin growth; orforglipron a watch item | Adjacent — frontier moving to oral agents |
| Pharmacy & Retail | ● High | Private-pay tirzepatide economics; PBS vs private cost gap | Direct — margin & affordability now |
| Consumer & Supplements | ● Medium | GLP-1 support supplements go mainstream in consumer health | Emerging — positioning opportunity |
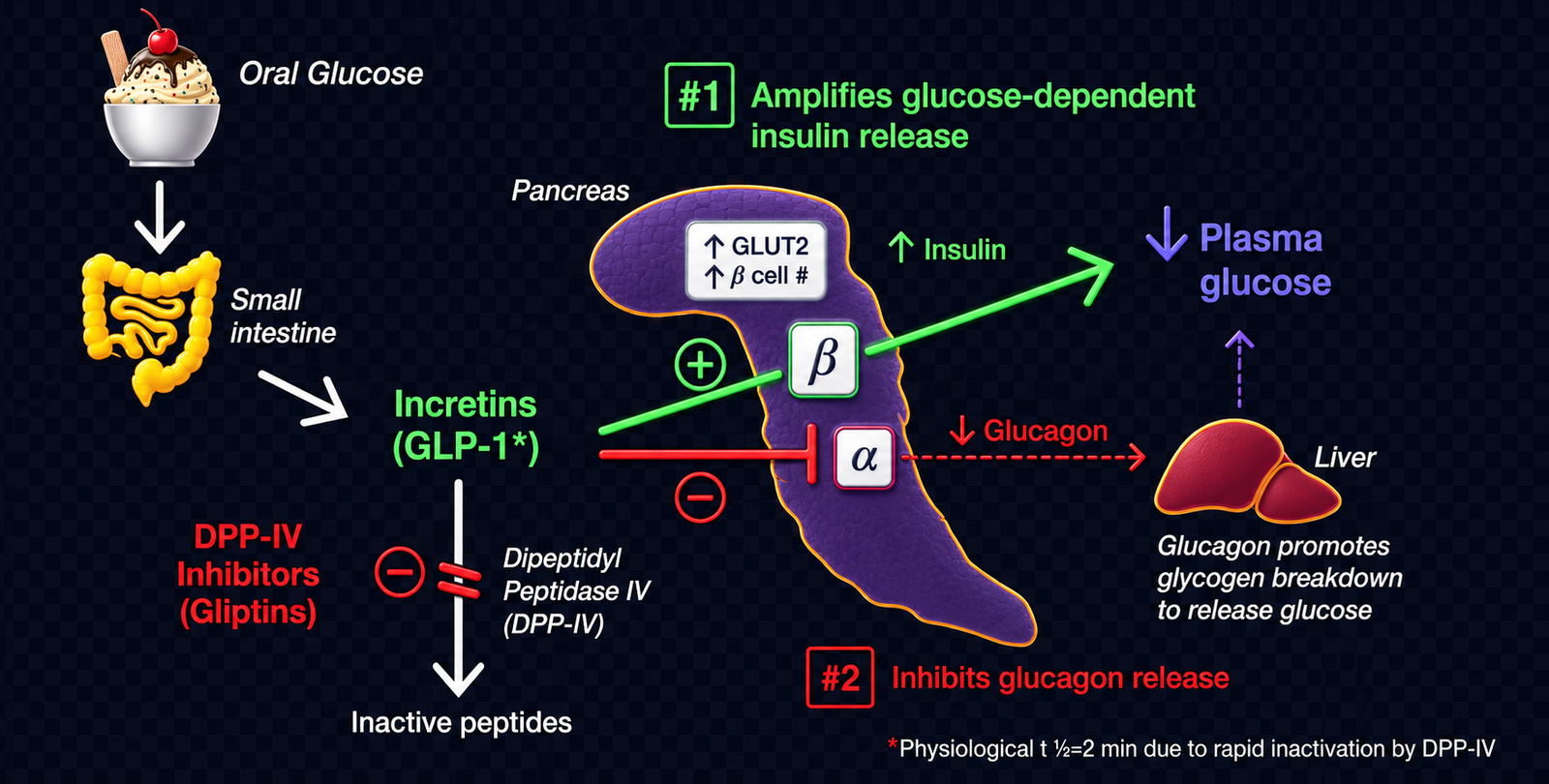
A plain-English explainer for readers who want the mechanism behind the market shift.
PBS, TGA, PBAC decisions, scheduling changes, and reimbursement pathway developments.
The PBAC recommended tirzepatide (Mounjaro, Eli Lilly) for adults with inadequately controlled type 2 diabetes, but Eli Lilly declined to proceed with a PBS listing under the proposed reimbursement conditions. Medicines Australia publicly attributed the failure to list to a "broken" PBS process, and reporting cited a Lilly estimate that around 450,000 Australians with type 2 diabetes would have benefited from subsidised access. The decision keeps tirzepatide a private-prescription medicine in Australia and leaves Ozempic (semaglutide) and Trulicity (dulaglutide) as the PBS-subsidised GLP-1 options for diabetes. (Sources: ABC News 28 Apr 2026; supporting coverage from AusDoc, RACGP newsGP, and Pharmacy Daily, 24–28 Apr 2026.)
The PBS Medicine Status page for semaglutide (information current as at 1 May 2026) shows Wegovy for established cardiovascular disease with obesity carries a PBAC recommendation (from the November 2025 meeting), but agreement on listing arrangements and a final PBS listing have not yet occurred. The status sits between recommendation and listing — a notice-of-intent stage rather than an active subsidy. (Source: PBS Medicine Status, SEMAGLUTIDE, current as at 1 May 2026.)
The PBAC's published advice on equitable access to GLP-1 obesity treatments identifies priority access groups — including patients with established cardiovascular disease, Aboriginal and Torres Strait Islander patients with obesity-related comorbidities, syndromic obesity, medication-induced obesity, and patients requiring weight loss ahead of surgery. The framing favours a managed, criteria-based rollout rather than open obesity subsidy. (Source: PBS, "PBAC advice on equitable access to GLP-1 obesity treatments".)
TGA shortage status, supply transitions, compounding enforcement, and grey-market integrity.
The TGA states the Ozempic (semaglutide) shortage has resolved, and that both new and existing patients can be prescribed and access treatment. A presentation transition remains in train: the 1.5 mL (0.25 mg / 0.5 mg) pre-filled pen is in PBS "Supply Only" status until 1 June 2026 and is being replaced by the 3 mL presentation. (Source: TGA, "Ozempic (semaglutide) supply information".)
TGA shortage information indicates the Trulicity (dulaglutide, Eli Lilly) shortage is expected to continue until 30 June 2026. Even with Ozempic normalised, this keeps a diabetes GLP-1 supply constraint live for prescribers and pharmacies. Recheck the TGA shortage page immediately before publication — shortage end-dates are routinely revised. (Source: TGA, "About the Trulicity (dulaglutide) shortage".)
As official supply improves, demand may shift away from grey-market and compounded pathways — but counterfeit product and inappropriate online prescribing remain ongoing risks. Compounded GLP-1 RA products have been prohibited from pharmacist compounding/supply since the regulatory amendments effective October 2024, and the TGA continues to publish GLP-1 safety and supply guidance. [Watch item — no new May 2026 compounding rule is implied here; this is context, pending any fresh TGA enforcement action.] (Sources: TGA GLP-1 safety and shortage pages; prior compounding-enforcement history.)
Semaglutide and tirzepatide patent expiries, generic applications, and Australian timeline implications.
No new Australian generic semaglutide approval or PBS listing occurred during this period. Australia's semaglutide secondary and formulation patent protections run into the 2030s, so generic semaglutide cannot legally enter Australian PBS channels in the near term. This window's access disruption is driven by reimbursement (the Mounjaro stand-off) and supply transitions — not by local generic substitution. [Australian timeline note: confirmed branded market; generic entry remains a 2030s-horizon event.]
The global semaglutide patent picture established earlier in 2026 — core patent expiries in India and China, and a wave of low-cost generic supply in those markets — remains the backdrop against which PBAC and sponsors negotiate. No new verified, Australia-relevant country-specific generic event arose in this particular window beyond that established context. The relevance to Australia is indirect: global price compression strengthens PBAC's cost-effectiveness arguments over time. [Australia timeline: patents to the 2030s; this is a pricing-narrative signal, not a near-term supply event.]
Company results, pipeline progress, new agents, and reporting discipline on approvals.
Eli Lilly's first-quarter 2026 results reported continued strong incretin growth: worldwide Mounjaro revenue of $8.7 billion (up 125% year on year) and US Zepbound revenue of $4.1 billion (up 79% year on year), alongside pipeline and regulatory updates spanning the oral GLP-1 orforglipron, the triple agonist retatrutide, and combination programs. The franchise momentum sits against Lilly's decision not to list Mounjaro on the Australian PBS — global volume growth does not depend on Australian subsidy. (Source: Eli Lilly, "Lilly reports first-quarter 2026 financial results".)
Reporting discipline note: the FDA approved orforglipron as Foundayo on 1 April 2026 for adults with obesity (or overweight with weight-related comorbidities) in the United States, per Eli Lilly's own announcement. That US approval does not extend to Australia, but the local pathway has opened: the TGA accepted Eli Lilly Australia's registration application for orforglipron calcium — proposed product name NEXVOUND, for obesity/overweight and type 2 diabetes — for evaluation in January 2026 (TGA "prescription medicines under evaluation"). On the evidence confirmed for this period, orforglipron is therefore a clinical and regulatory watch item here — an oral GLP-1 that is US-approved and now under active TGA evaluation, but not yet entered on the ARTG (registered) or PBS-listed as an Australian product. [Watch item — verify ARTG registration before asserting Australian availability.]
Pharmacy economics, dispensing channel, and the affordability frame for private-pay metabolic medicine.
With Lilly declining to proceed with a Mounjaro PBS listing, tirzepatide stays outside PBS co-payment access and remains a private-prescription medicine — indicatively in the order of several hundred dollars per month, depending on dose and pharmacy. The dispensing volume, margin, patient affordability, counselling burden, and retention pathways therefore stay tied to the private channel rather than to subsidised PBS scripts. (Sources: ABC News 28 Apr 2026; indicative private pricing consistent with prior-issue market data.)
PBS-listed medicines are supplied at co-payments cited in Australian reporting as around $25 (general) and $7.70 (concession), while non-listed private GLP-1 medicines remain full out-of-pocket. That contrast — a capped co-payment versus a several-hundred-dollar monthly private price — is the single clearest frame for how access economics now shape GLP-1 demand. (Source: ABC News 28 Apr 2026.)
Consumer awareness, supplement category shifts, and the pharmacy permission space for GLP-1 support.
Mainstream consumer-health coverage in late April 2026 framed a GLP-1 "support stack" around protein, fibre, probiotics, multivitamins, muscle preservation, addressing nutrient gaps, easing constipation, and tolerability support — alongside balanced diet and strength training. The signal here is mainstreaming of the category in consumer media, not new clinical authority. (Source: Healthline, "Best Supplements to Support GLP-1s", 28 Apr 2026 — used as a mainstreaming signal, not a clinical reference.)
[Analysis] Grocery can win the high-protein and high-fibre functional-food opportunity, but pharmacy has the stronger permission space for pharmacist-guided supplement bundles and tolerability counselling tied to a GLP-1 prescription. As supplement content mainstreams, the differentiated position is clinical guidance — matching products to a patient's regimen and side-effect profile — rather than shelf presence alone. This item is framed as analysis, not a sourced market event.
The Mounjaro stand-off, not a new launch, is the defining event of this period — and it redraws the access map. The PBAC recommended tirzepatide for inadequately controlled type 2 diabetes, but Eli Lilly declined to proceed with PBS listing under the proposed reimbursement conditions. With Lilly's global incretin franchise still compounding (Mounjaro $8.7B and Zepbound $4.1B in Q1 2026), the company has little pressure to accept Australian terms it considers unfavourable. The practical message for pharma commercial directors, pharmacy buyers, and investors: premium GLP-1 access in Australia will be settled by reimbursement negotiation over multiple years, and a clinically superior medicine can remain a private-pay product for an extended period.
Wegovy's staged pathway shows what "access" will actually look like — narrow and criteria-based. Wegovy carries a PBAC recommendation for established cardiovascular disease with obesity but is not yet listed, and the PBAC's equitable-access advice points to priority groups rather than open obesity subsidy. Anyone planning around a broad consumer obesity reimbursement should recalibrate: the near-term reality is defined cohorts, eligibility screening, and managed rollout. Patient-support and prescriber-education investments should be built for criteria-based access.
Supply has normalised, so the operational task moves from scarcity to discipline. The TGA reports the Ozempic shortage resolved, but the 1.5 mL starter pen remains PBS Supply Only until 1 June 2026 during a 3 mL transition, and the Trulicity shortage runs to 30 June 2026. For pharmacies, the risk is no longer "can we get stock" but "are we dispensing the right presentation and counselling the change correctly." Recheck both TGA pages before acting — shortage and transition dates are revised frequently.
Private-pay economics now sit at the centre of the pharmacy GLP-1 story. With tirzepatide outside PBS co-payment access and a stark gap between PBS co-payments (~$25 general / $7.70 concession) and full private monthly prices, affordability segmentation will increasingly determine initiation, persistence, and switching. Pharmacies that build retention support, affordability options, and structured counselling around private-pay GLP-1 dispensing will defend both margin and adherence better than those treating it as a transactional fill.
The consumer "GLP-1 support" category is mainstreaming — and pharmacy holds the most defensible position to own it. Protein, fibre, probiotic, and micronutrient support content is now mainstream consumer-health material. Grocery can win functional foods, but pharmacy's permission space for pharmacist-guided bundles and tolerability counselling is stronger. The constraint is compliance: brands and pharmacies must frame around nutrition adequacy and support, never around treating or preventing GLP-1 adverse effects. Those that get the positioning right capture a high-trust, durable adjacency to the prescription itself.